Pars Plana Vitrectomy (PPV)
Micro-incision vitreous removal with direct surgical access to the vitreoretinal interface — the definitive procedure for retinal detachment, macular hole, epiretinal membrane, and a broad range of posterior segment diseases.
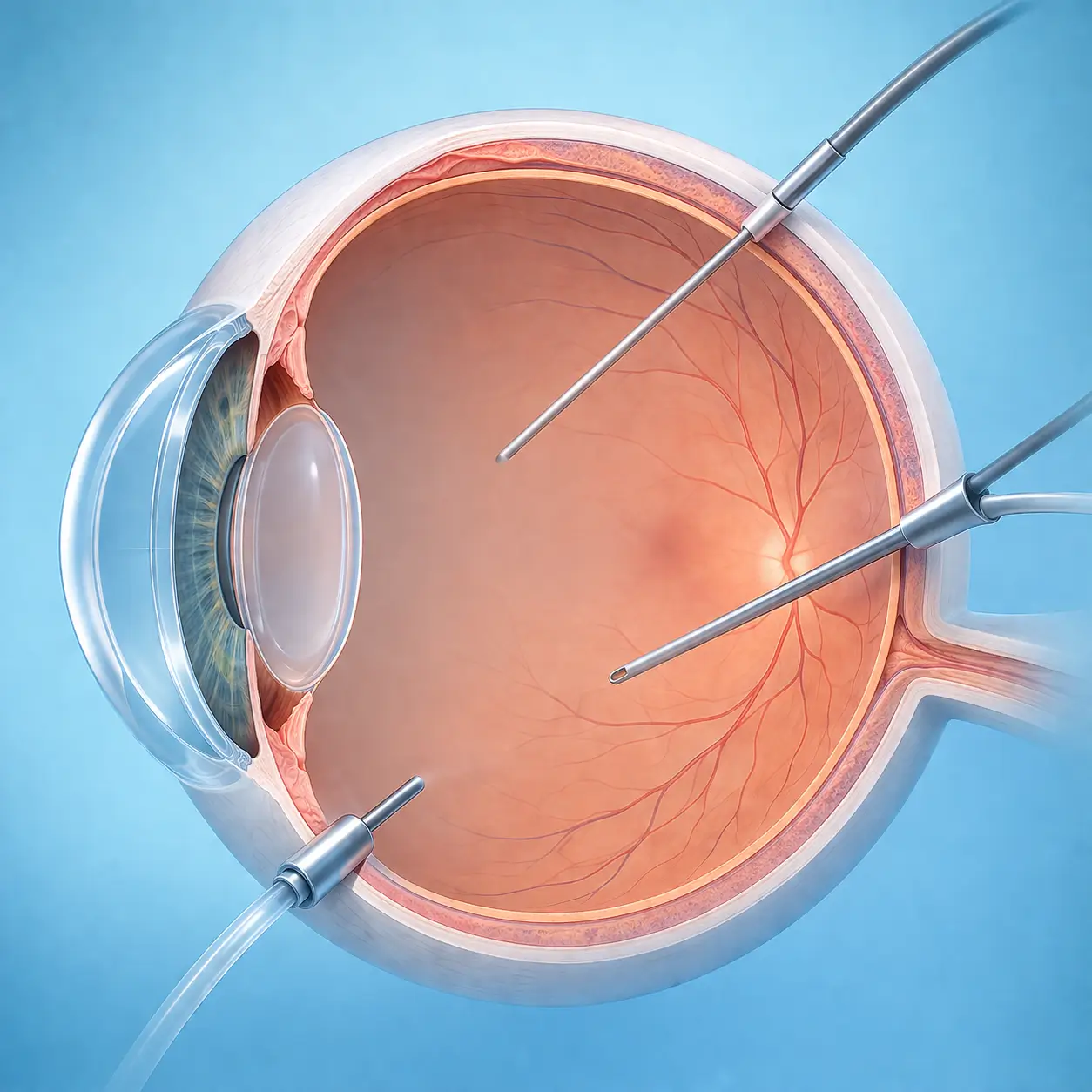
Pars Plana Vitrectomy (PPV) is the foundational surgical procedure for posterior segment diseases. Three micro-incision ports are created at the pars plana (3.5-4 mm posterior to the limbus) using 23G, 25G, or 27G trocar cannula systems. A vitreous cutter, infusion cannula, and endoilluminator are inserted, enabling the surgeon to remove the vitreous gel and directly address pathology at the vitreoretinal interface under high-magnification microscopy and wide-field endoillumination. Contemporary small-gauge (25G/27G) systems create incisions of only 0.5-0.7 mm that are typically self-sealing, dramatically reducing surgical trauma and speeding recovery. The indications for PPV are extensive: rhegmatogenous retinal detachment (especially with proliferative vitreoretinopathy or giant tears), tractional retinal detachment (diabetic, RVO-related), macular hole (with internal limiting membrane peeling to promote closure), epiretinal membrane (membrane peeling), vitreous hemorrhage, intraocular foreign body removal, infectious endophthalmitis, and symptomatic vitreous floaters (floaterectomy). At procedure completion, an intraocular tamponade agent is typically instilled — air, SF6 gas, C3F8 gas, or silicone oil — to support retinal reattachment. Gas tamponade requires strict postoperative face-down or disease-specific positioning until absorption (SF6 ~2 weeks; C3F8 ~6-8 weeks). Silicone oil requires a planned secondary removal procedure at 3-6 months.
Quick Reference
Treatment
1 hours – 3 hours
Observation
1 days – 0.2 months
Est. Cost
$3,200 – $10,000
Department
Ophthalmology
Who Is This For
Is Pars Plana Vitrectomy (PPV) Right for You?
Good Candidates
- Rhegmatogenous retinal detachment — especially with PVR, giant retinal tear, or posterior pole breaks
- Tractional retinal detachment (diabetic or RVO-related)
- Full-thickness macular hole (stage II-IV)
- Epiretinal membrane with significant vision loss or metamorphopsia
- Vitreous hemorrhage not clearing with observation, or associated with retinal detachment requiring urgent surgery
- Severely symptomatic vitreous opacities (dense floaters, amyloid deposition)
May Not Be Suitable
- Systemic condition precluding surgical anesthesia (requires medical optimization before proceeding)
- Active intraocular infection (except endophthalmitis where vitrectomy is the treatment)
- Severe corneal opacity limiting surgical visibility (corneal surgery may be needed first)
- Inability to comply with required postoperative positioning (e.g., face-down for macular hole — requires individual assessment in elderly patients or those with cervical disease)
- End-stage retinal disease with minimal visual potential (individual risk-benefit evaluation required)
Step-by-Step Process
How Pars Plana Vitrectomy (PPV) Works
Anesthesia and Positioning
Anesthesia is chosen based on surgical complexity and patient cooperation: peribulbar or retrobulbar block for cooperative adults; general anesthesia for children, uncooperative patients, or anticipated operative duration >2 hours. The patient lies supine with the head stabilized.
Three-Port Setup
Three trocar cannulas (23G/25G/27G) are inserted at the pars plana (3.5-4 mm posterior to the limbus): an infusion cannula inferiorly for IOP maintenance, and two instrument ports superotemporally and supranasally. Infusion is activated and confirmed flowing freely into the vitreous cavity.
Core and Peripheral Vitrectomy
A wide-field visualization system (BIOM or RESIGHT) is attached. Under bright endoillumination, the high-speed vitreous cutter (5,000-10,000 rpm) removes central and peripheral vitreous gel systematically, simultaneously clearing hemorrhage, inflammatory cells, or opacities.
Retinal and Interface Management
Disease-specific steps are performed: Macular hole/ERM — triamcinolone-assisted ILM or membrane staining, then microforceps peeling; Retinal detachment — perfluorocarbon liquid (PFCL) injection to flatten the retina, break treatment by endolaser, subretinal fluid drainage; Diabetic tractional membrane — staged delamination and segmentation of fibrovascular proliferation to relieve traction.
Tamponade and Wound Closure
Fluid-air exchange replaces PFCL if used; tamponade agent is then injected (air, SF6, C3F8 gas, or silicone oil depending on diagnosis and retinal status). Trocar cannulas are removed; 25G/27G wounds typically self-seal without sutures. Subconjunctival antibiotic and steroid injection, antibiotic ointment, and eye patch are applied.
Postoperative Positioning Instruction
Macular hole patients immediately begin face-down positioning. Retinal detachment patients assume the position that keeps the gas bubble in contact with the treated break. Nurses provide detailed, confirmed instruction before the patient leaves the operating suite.
PPV is a single procedure, though secondary surgery may be needed (silicone oil removal at 3-6 months; repeat PPV for complex retinal re-detachment). Postoperative antibiotic, steroid, and mydriatic drops are required for 4-6 weeks.
Cost Information
Cost Estimate for Pars Plana Vitrectomy (PPV)
Estimated Price Range
$3,200 – $10,000
What's Included
Public tier-3A International Medical Department: 25G micro-incision vitrectomy (retinal detachment) including hospitalization approximately ¥22,000-35,000; complex cases (PDR with tractional detachment, silicone oil fill) including hospitalization approximately ¥35,000-55,000. Premium private eye centers: micro-incision vitrectomy (retinal detachment/macular hole) full course approximately ¥40,000-70,000, with private room, ample surgical time, senior specialist as primary surgeon, and detailed postoperative management.
Before Your Visit
What to Prepare
Required Tests & Examinations
If you already have recent valid test results, bring the reports. If not, these assessments can usually be completed in China before the procedure.
Macular OCT (assess retinal structure, vitreoretinal interface status, detachment extent)
B-scan ocular ultrasound (assess vitreous and retinal status, essential when media are opaque)
Fundus fluorescein angiography (FFA — evaluate retinal vasculature; mandatory before diabetic PPV)
Axial length and keratometry (for high myopia assessment; IOL calculation if silicone oil removal is planned)
Intraocular pressure measurement
Systemic preoperative screening (ECG, CBC, coagulation, blood glucose)
Documents & Materials to Bring
Required to Bring
Recent fundus OCT, B-scan, and FFA reports
Medical history (diabetes control is especially critical)
Anticoagulant medication records (aspirin, warfarin — perioperative management plan needed)
Prior ocular surgery records
Passport and valid visa
Companion & Support
Hospitalization of 3-7 days (longer for complex cases) is required, and family caregiver presence is essential — particularly to assist with face-down positioning for macular hole (5-7 days of face-down posturing severely limits daily function and requires dedicated caregiver support). Continued accompaniment to outpatient follow-up visits is also important.
After Treatment
Recovery & Follow-Up
Strict adherence to the prescribed postoperative positioning (face-down for macular hole — typically 5-7 days) is critical to surgical success; do not deviate from instructions
Do not board any aircraft while intraocular gas is present — altitude-related gas expansion can cause an acute IOP spike exceeding 60 mmHg, risking permanent vision loss
Very poor vision during the gas tamponade phase is normal; vision gradually improves as the gas absorbs
Apply all prescribed eye drops (antibiotic + mydriatic + steroid) strictly for 4-6 weeks
Avoid strenuous activity, bending at the waist, and heavy lifting for at least 1 month
Seek immediate attention for sudden vision loss, a dramatic increase in floaters, or worsening redness
Follow-Up Schedule
Follow-up at day 1, day 3, week 1, week 2 (assess gas absorption), month 1, and month 3. Patients with silicone oil are scheduled for oil removal surgery at 3-6 months.
Related Conditions
Conditions This Procedure Treats
Ready to Plan Pars Plana Vitrectomy (PPV) in China?
Let Carevia help you find the right hospital, coordinate your treatment, and arrange every detail of your medical trip.
Frequently Asked Questions
Need personalized guidance?
Our care coordinators can help you assess whether this procedure fits your situation.
Contact Us