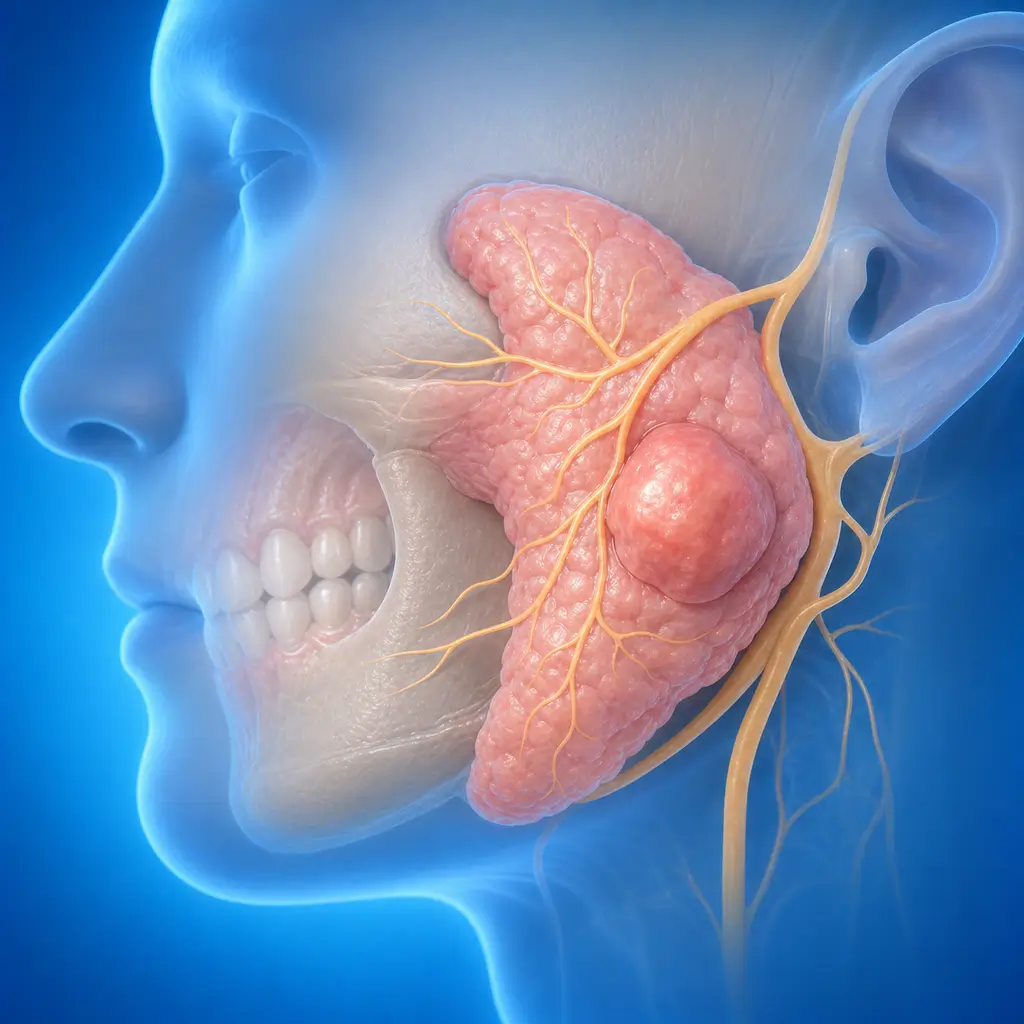
Salivary gland tumor
Salivary gland tumors are benign or malignant tumors arising from salivary glands. They most commonly occur in the parotid gland. Most are benign, but some have recurrence or malignant transformation potential, and surgical excision is the main treatment.
Common Symptoms
Recognizing Salivary gland tumor
Focus on the most useful decision cues first: common symptoms, the patients or situations that usually prompt review, and any signs that need faster assessment.
Common Symptoms
Signs patients often notice before evaluation
Benign tumors: painless, slow-growing mass over months to years. Borders are clear, texture is medium or firm, mobility is good, and there is no facial nerve paralysis. Benign parotid tumors are located below the earlobe or in front of the tragus, benign submandibular tumors in the submandibular triangle, and minor salivary gland tumors under the oral mucosa
Malignant tumors: faster-growing mass, pain, unclear borders, fixation, and adhesion to surrounding tissues. Facial nerve paralysis, skin ulceration, bleeding, and regional lymph node enlargement may occur. Adenoid cystic carcinoma has a tendency for perineural invasion and can spread along nerves, causing early pain and numbness. Mucoepidermoid carcinoma may be cystic and grow relatively slowly
When to Seek Evaluation
Typical patients and situations that warrant review
Pleomorphic adenoma is more common at ages 30-50
Warthin tumor is more common in middle-aged and older male smokers
Malignant tumors can occur at any age
A painless mass appears in the parotid area, submandibular area, or under the oral mucosa
A mass rapidly enlarges over a short time, becomes painful, causes facial nerve paralysis, or causes skin ulceration
Imaging finds a salivary gland space-occupying lesion
Urgent Assessment
If a salivary gland region mass grows rapidly over a short time, is painful, has unclear borders, causes skin ulceration, facial paralysis, numbness, limited mouth opening, or neck lymph node enlargement, seek evaluation promptly in oral and maxillofacial surgery or a head and neck oncology specialty to exclude malignancy.
Treatment Approaches
Treatment Directions for Salivary gland tumor
Salivary gland tumors usually require planning based on imaging and fine-needle aspiration/pathology results and cannot be judged as benign or malignant by palpation alone
Benign tumors are usually treated mainly by complete surgical excision, with the surgical extent depending on tumor site, size, and relationship to the facial nerve or duct
For suspected or pathologically confirmed malignancy, surgical extent, neck management, postoperative radiotherapy, and other comprehensive treatment are determined by stage, pathology type, nerve invasion, and lymph node status
Recurrent tumors, deep-lobe parotid tumors, sublingual or minor salivary gland tumors, or tumors with facial nerve symptoms should be evaluated by a head and neck tumor multidisciplinary team
What usually shapes the treatment plan
Clinical Assessment
Key Assessments for Salivary gland tumor
These are the main areas doctors usually review first. If you already have relevant test or imaging reports, bring them to speed up the assessment. They are helpful but not required, and the same workup can also be completed in China.
Mass location
Size
Growth rate
Borders
Mobility and pain
Facial nerve function
Skin ulceration
Numbness and limited mouth opening
Cervical lymph nodes and risk of distant metastasis
Ultrasound
CT or MRI assessment of tumor extent and relationship to facial nerve/surrounding tissue
Fine-needle aspiration or pathology to determine benign or malignant nature and specific type
Before You Travel
How to Prepare
Bring previous systemic disease and treatment history, and recent imaging studies if available
Planning Notes
Pre-Assessment Required
Bring salivary gland ultrasound, contrast-enhanced CT or MRI, and fine-needle aspiration, core biopsy, or previous pathology reports if available. The doctor will combine imaging, facial nerve function, and pathology type to determine surgical extent, whether the facial nerve can be preserved or needs treatment, whether cervical lymph node management is needed, and whether postoperative radiotherapy is needed.
Remote Pre-Assessment
Intraoral photos, the course of pain/swelling, previous dental records, and imaging can be submitted remotely for preliminary triage, urgency assessment, and an estimated treatment direction. Final diagnosis still requires in-person intraoral examination and necessary imaging.
Multidisciplinary Assessment
For suspected malignancy, recurrence, facial nerve involvement, deep-lobe parotid disease, or skull base invasion, joint evaluation by oral and maxillofacial surgery, head and neck oncology, imaging, pathology, radiation oncology, and rehabilitation/prosthodontic teams is recommended.
Medical History Important
Previous dental treatment history, imaging, allergy history, anticoagulant/bisphosphonate use, diabetes, and immune-related diseases can affect diagnosis, anesthesia, bleeding and infection risk, and treatment selection.
Ready to Explore Treatment for Salivary gland tumor?
Let Carevia help you connect with the right specialists, compare hospitals, and plan your medical trip to China.