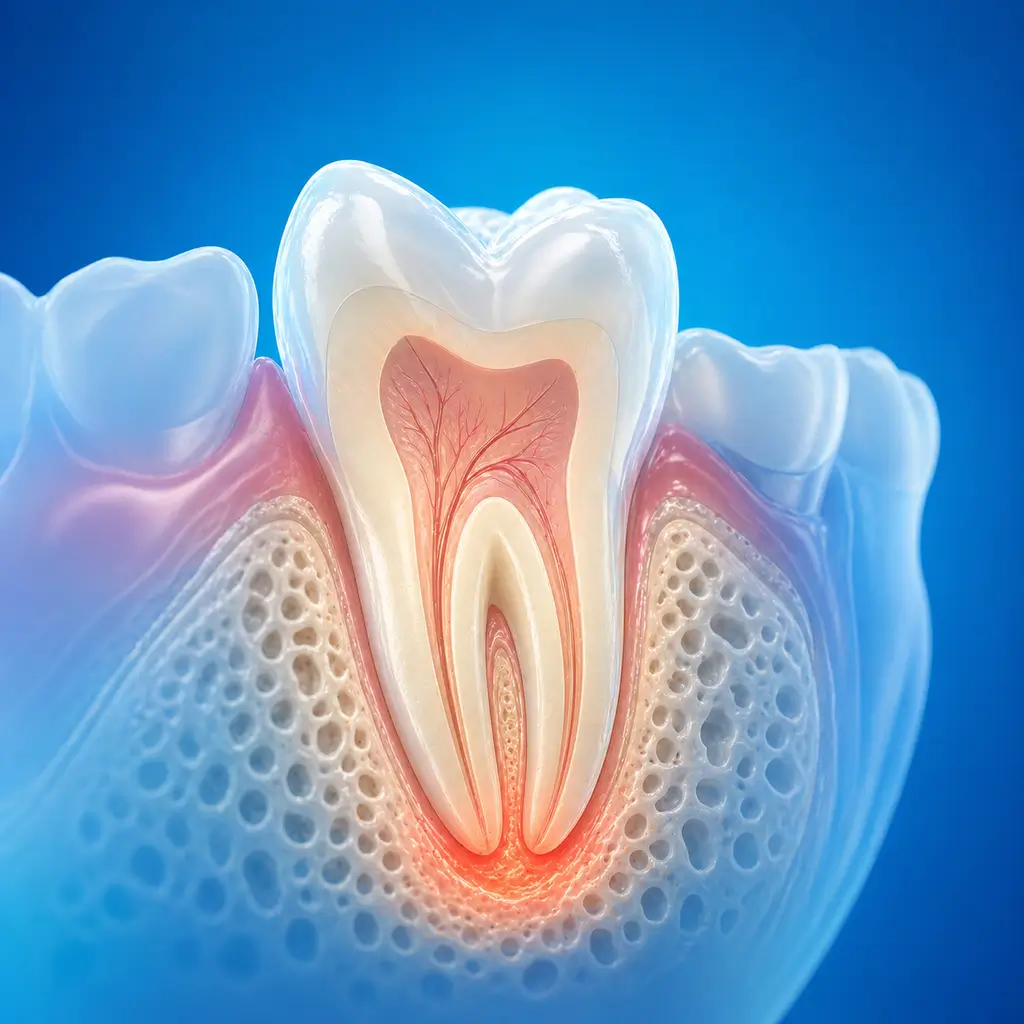
Periapical periodontitis
Periapical periodontitis is inflammation of the tissues around the tooth root apex, including cementum, periodontal ligament, and alveolar bone. It is often secondary to pulp infection and can usually be treated effectively, such as with root canal treatment, to preserve the tooth.
Common Symptoms
Recognizing Periapical periodontitis
Focus on the most useful decision cues first: common symptoms, the patients or situations that usually prompt review, and any signs that need faster assessment.
Common Symptoms
Signs patients often notice before evaluation
Acute periapical periodontitis: pain when biting on the affected tooth, which can usually be accurately located. In the acute serous phase, the tooth root may feel itchy, or only mild pain occurs during biting
In the acute suppurative phase, persistent spontaneous dull pain occurs and worsens with biting. The affected tooth may feel elongated and painful when contacting the opposing tooth. As the disease progresses, apical abscess, subperiosteal abscess, or submucosal abscess may occur, with redness, swelling, tenderness, regional lymph node enlargement and tenderness, and in severe cases fever, chills, and other systemic symptoms
Chronic periapical periodontitis: usually has no obvious subjective symptoms. Some affected teeth have mild discomfort or weak biting during chewing. Typical signs include a draining sinus tract on the gingiva corresponding to the affected tooth, with pus expressed on pressure
After pulp necrosis, the tooth gradually loses luster and becomes gray or darker
The affected tooth may have mild percussion pain or mobility. Chronic periapical periodontitis can acutely flare when immunity is reduced, causing swelling and pain
When to Seek Evaluation
Typical patients and situations that warrant review
Common in patients with a history of pulp disease, especially untreated caries or persistent pulpitis. It is also common in patients with dental trauma or inappropriate dental treatment history. It can occur at any age
Persistent or recurrent tooth pain that gradually worsens
Pain or discomfort when biting or chewing
Redness, swelling, or pus discharge from the gum near the root apex
Tooth abnormalities such as crown discoloration or caries
Oral examination shows tooth mobility, percussion pain, or abnormal gingival swelling
Physical examination shows enlarged and painful mandibular or submental lymph nodes
Urgent Assessment
Acute periapical periodontitis should be evaluated promptly if severe biting pain, a feeling that the tooth is elongated, gingival or facial swelling, fever, limited mouth opening, or swelling that worsens after pain decreases occurs. If infection continues to spread, maxillofacial space infection or sepsis may develop.
Treatment Approaches
Treatment Directions for Periapical periodontitis
Root canal treatment
For acute periapical periodontitis, access opening and drainage are performed first to relieve pain and pressure, with incision and drainage when necessary
For failed root canal treatment, large periapical cysts, or anatomically complex cases, periapical surgery may be considered
If the tooth has no retention value, extraction is needed
What usually shapes the treatment plan
Clinical Assessment
Key Assessments for Periapical periodontitis
These are the main areas doctors usually review first. If you already have relevant test or imaging reports, bring them to speed up the assessment. They are helpful but not required, and the same workup can also be completed in China.
Course type, acute or chronic, and pathological type, such as serous, suppurative, granuloma, abscess, or cyst
Whether periapical bone destruction is present and its extent
Pulp vitality status of the affected tooth
Whether a sinus tract has formed
Whether the affected tooth can be retained
Overall health status, especially diabetes, immune status, and coagulation function
Before You Travel
How to Prepare
Maintain good oral cleanliness
Bring previous dental records, especially radiographs and root canal treatment records
Planning Notes
Pre-Assessment Required
An oral specialist should perform an intraoral examination and, as appropriate, periodontal probing, pulp vitality testing, periapical radiographs, panoramic radiographs, or CBCT before determining the treatment plan. Key checks include specialist oral examination: percussion to assess the presence and degree of tenderness; probing to check for deep caries and pulp exposure; visual inspection for gingival redness, swelling, sinus tract, and purulent discharge; and tooth mobility testing. Bring imaging and pulp vitality test results if available.
Remote Pre-Assessment
Intraoral photos, the course of pain/swelling, previous dental records, and imaging can be submitted remotely for preliminary triage, urgency assessment, and an estimated treatment direction. Final diagnosis still requires in-person intraoral examination and necessary imaging.
Multidisciplinary Assessment
Medical History Important
Previous dental treatment history, imaging, allergy history, anticoagulant/bisphosphonate use, diabetes, and immune-related diseases can affect diagnosis, anesthesia, bleeding and infection risk, and treatment selection.
Ready to Explore Treatment for Periapical periodontitis?
Let Carevia help you connect with the right specialists, compare hospitals, and plan your medical trip to China.