Scleral Buckling Surgery
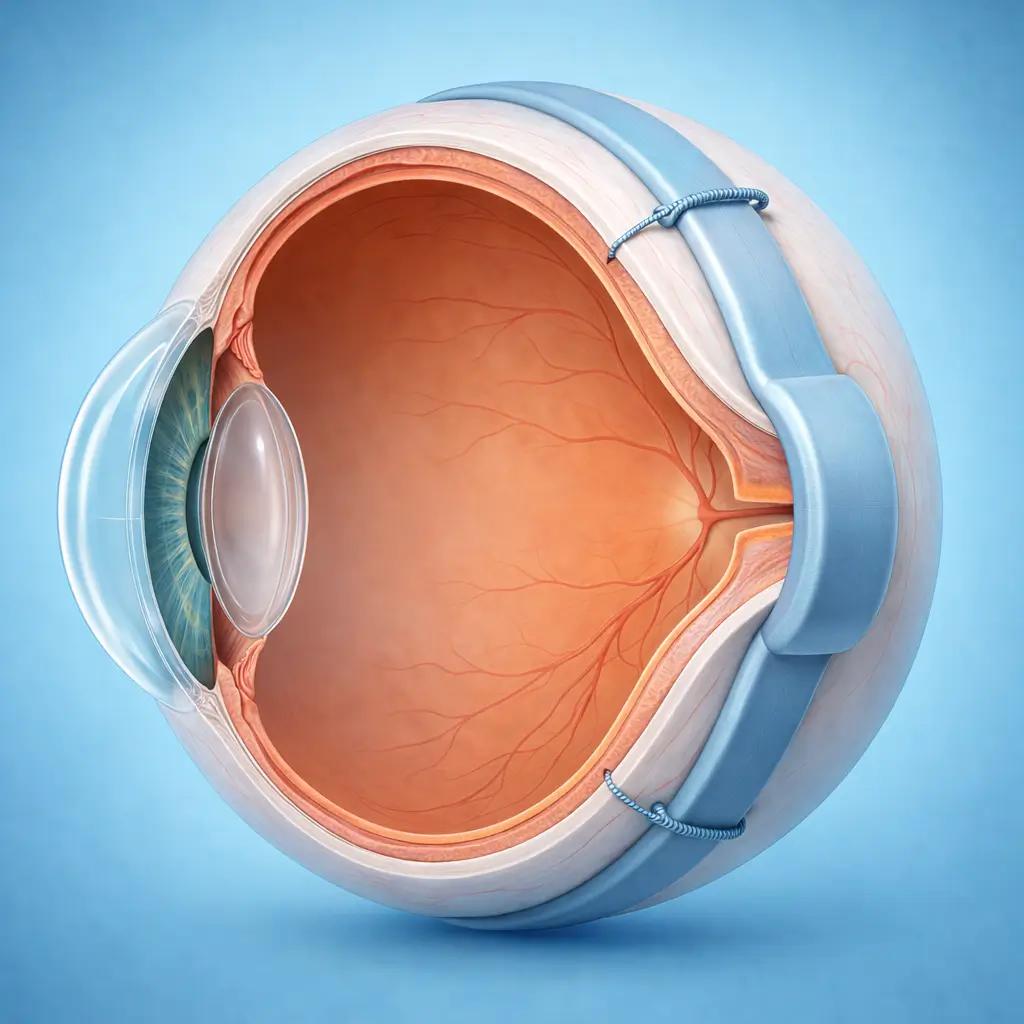
Silicone bands or sponges are sutured to the outer scleral surface to indent the eye wall, bringing the retinal break into contact with the underlying pigment epithelium and sealing the detachment — the classic external approach to retinal detachment repair without entering the vitreous cavity.
Scleral buckling (SB) is the time-honored external surgical approach to rhegmatogenous retinal detachment (RRD). Silicone explants (sponge, segmental band, or encircling band) are sutured to the outer scleral surface, creating an indentation that brings the detached retinal break into apposition with the retinal pigment epithelium, eliminating the hydrostatic force driving fluid through the break. Cryotherapy or laser retinopexy seals the break, and anatomic reattachment is achieved. Scleral buckling preserves the integrity of the vitreous cavity, avoids the cataract acceleration associated with vitrectomy, and requires no intraocular tamponade — making it especially advantageous for phakic young patients who retain accommodative capacity. Single-surgery anatomic success rates (70-80%) and ultimate reattachment rates (>90%) are comparable to vitrectomy, and costs are generally lower. SB is best suited for RRD with breaks anterior to or at the equator, absent or mild proliferative vitreoretinopathy (PVR ≤ Grade B), no significant vitreous hemorrhage, and clearly localizable breaks — particularly in young phakic patients. Posterior breaks, severe PVR, giant tears, or complex detachments with macular involvement generally favor vitrectomy.
Quick Reference
Treatment
1 hours – 2 hours
Observation
1 days – 3 days
Est. Cost
$1,900 – $5,900
Department
Ophthalmology
Who Is This For
Is Scleral Buckling Surgery Right for You?
Good Candidates
- Rhegmatogenous retinal detachment with breaks at or anterior to the equator and no significant vitreous hemorrhage
- Young phakic patients (preserves accommodative function; avoids cataract acceleration)
- RRD with mild PVR (Grade B or less)
- Single or multiple localized, clearly identifiable breaks
- Patients who are not candidates for or prefer to avoid vitrectomy
May Not Be Suitable
- Severe proliferative vitreoretinopathy (PVR Grade C or higher)
- Posterior pole breaks near the macula (difficult to effectively support with a buckle)
- Giant retinal tears (>90°)
- Dense vitreous hemorrhage preventing break localization
- Heavy conjunctival scarring from multiple prior episcleral surgeries
Step-by-Step Process
How Scleral Buckling Surgery Works
Anesthesia
Peribulbar block or general anesthesia (preferred for children and uncooperative patients). The patient lies supine; the surgical eye is sterilized and draped.
Conjunctival Opening and Break Localization
A 360° conjunctival peritomy exposes the sclera. The four rectus muscles are isolated and controlled with traction sutures to allow full globe rotation. Under indirect ophthalmoscopy with scleral depression, each retinal break is localized to its corresponding scleral surface position and marked.
Cryotherapy to Retinal Breaks
A cryotherapy probe is applied to each marked site. Under indirect ophthalmoscopic visualization, cryotherapy is applied to the edges of each break (-60°C; a white retinal reaction confirms adequate treatment), creating an adhesive chorioretinal scar that will permanently seal the break upon healing.
Buckle Placement and Fixation
An appropriate explant is selected (silicone sponge for segmental buckling; silicone band or encircling tire for circumferential buckling) based on break number and distribution. The explant is placed over the marked scleral positions and fixed with non-absorbable sutures (5-0 Mersilene or titanium). Position is confirmed to provide full coverage of all breaks.
Subretinal Fluid Drainage and IOP Adjustment (if needed)
If subretinal fluid prevents break apposition, controlled external drainage through a sclerotomy releases subretinal fluid to facilitate reattachment. Sterile air or BSS may be injected to normalize IOP.
Conjunctival Closure and Completion
Rectus muscles are repositioned and the conjunctiva is closed watertight. Subconjunctival antibiotic and steroid are injected; an eye pad is applied. Indirect ophthalmoscopy confirms satisfactory break apposition before the patient leaves the OR.
Scleral buckling is a single procedure. The silicone explant is permanently retained on the globe (removal is rarely needed unless buckle-related complications arise). Anti-inflammatory drops are used for 4-6 weeks postoperatively.
Cost Information
Cost Estimate for Scleral Buckling Surgery
Estimated Price Range
$1,900 – $5,900
What's Included
Public tier-3A International Medical Department: scleral buckling including hospitalization approximately ¥13,000-22,000; premium private eye centers: approximately ¥22,000-40,000, including comprehensive preoperative assessment (indirect ophthalmoscopy mapping, B-scan, OCT), surgery, and detailed postoperative management with senior retinal specialist and private room. Generally lower cost than vitrectomy.
Before Your Visit
What to Prepare
Required Tests & Examinations
If you already have recent valid test results, bring the reports. If not, these assessments can usually be completed in China before the procedure.
Indirect ophthalmoscopy with scleral depression — comprehensive mapping of detachment extent and break locations (the cornerstone of surgical planning)
B-scan ocular ultrasound (vitreous and retinal assessment, especially with media opacity)
Macular OCT (assess foveal involvement; predict visual prognosis)
Axial length (high myopia assessment)
Intraocular pressure
Systemic preoperative screening
Documents & Materials to Bring
Required to Bring
Fundus diagram from indirect ophthalmoscopy showing break locations
B-scan and OCT reports
Medical history and medication records
Passport and valid visa
Companion & Support
Hospitalization of 2-5 days is required; family caregiver support is essential. Reduced vision and periocular swelling limit independence during the early recovery period. Accompaniment to early outpatient follow-up is also recommended.
After Treatment
Recovery & Follow-Up
Eyelid swelling and restricted eye movement in the first few days are normal postoperative reactions and resolve within 2-3 weeks
Transient diplopia from extraocular muscle disturbance is common and typically improves within weeks
The buckle slightly increases axial length, causing a mild myopic shift — refraction should be rechecked once vision stabilizes and glasses updated if needed
Apply prescribed antibiotic, steroid, and mydriatic drops as directed; mydriasis reduces inflammation and prevents synechiae
Avoid vigorous activity and heavy lifting for 1 month
Vision recovery after reattachment is gradual; allow 3-6 months for stabilization
Follow-Up Schedule
Follow-up at day 1, week 1, week 2, month 1, and month 3; then every 6-12 months once reattachment is confirmed stable.
Related Conditions
Conditions This Procedure Treats
Ready to Plan Scleral Buckling Surgery in China?
Let Carevia help you find the right hospital, coordinate your treatment, and arrange every detail of your medical trip.
Frequently Asked Questions
Need personalized guidance?
Our care coordinators can help you assess whether this procedure fits your situation.
Contact Us