Lacrimal Probing and Intubation
A metal probe is used to open the blocked lacrimal drainage pathway; a silicone tube may be left in place to maintain patency. Primarily indicated for congenital nasolacrimal duct obstruction in infants and selected adults with lacrimal stenosis.
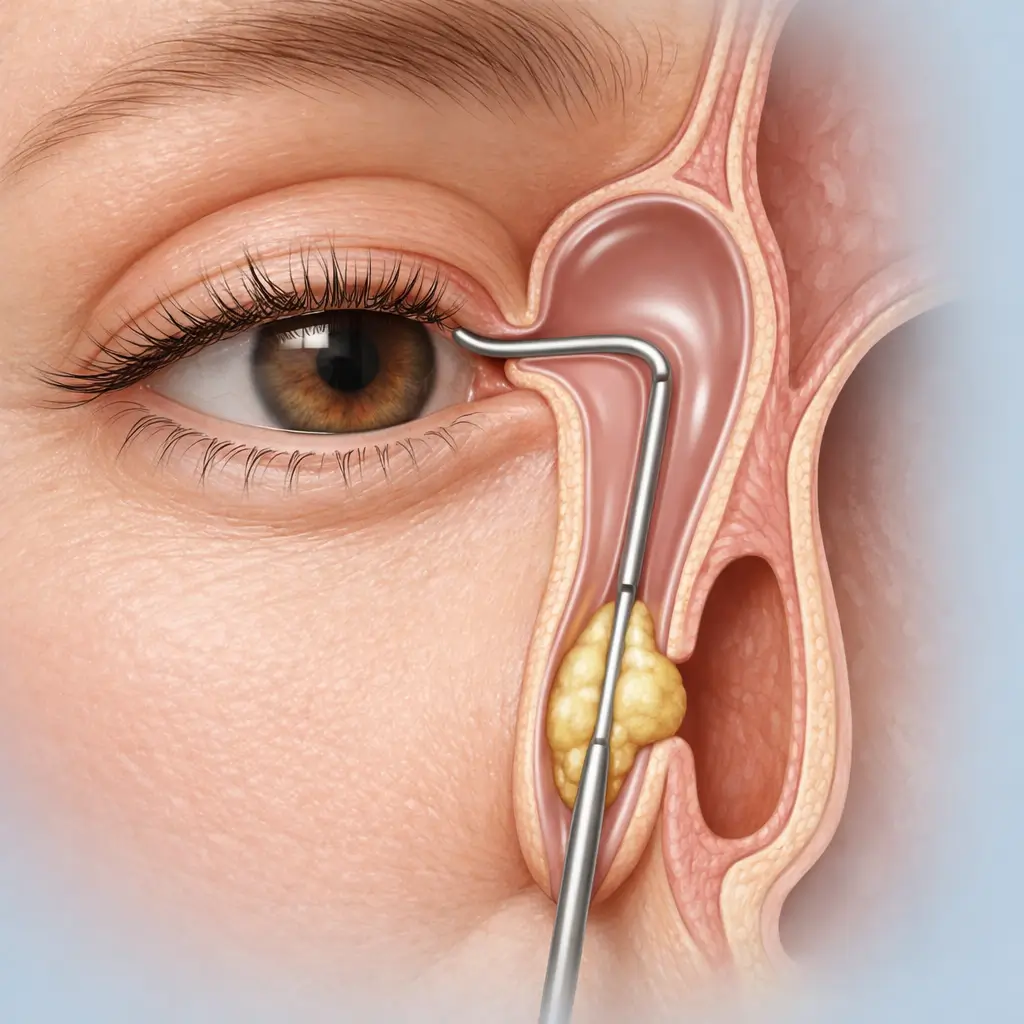
Lacrimal probing and intubation is the fundamental surgical intervention for lacrimal drainage obstruction, and the first-line procedure for congenital nasolacrimal duct obstruction (CNLDO). CNLDO most commonly results from a membranous obstruction (Hasner's valve) at the lower end of the nasolacrimal duct; the majority resolve spontaneously within 12 months. When conservative management (lacrimal sac massage) fails or the condition persists beyond 12-18 months, surgical probing is recommended. The procedure uses a fine Bowman probe inserted through the lacrimal punctum, advanced through the canaliculus and lacrimal sac, and directed inferiorly to perforate the obstructing membrane and enter the nasal cavity. If the obstruction is severe, the canal is unstable post-probing, or in adult cases of lacrimal stenosis, a silicone tube (e.g., Crawford or monocanalicular tube) is co-inserted to maintain luminal patency for 3-6 months before elective removal. Pediatric cases are performed under general anesthesia (inhalation induction; typically 5-15 minutes) for safe cooperation. Older children and adults may be managed under topical and local infiltration anesthesia. First-tier city children's hospitals and Tier-3A ophthalmology centers report CNLDO probing success rates of 90-95% in infants aged 12-24 months.
Quick Reference
Treatment
10 mins – 20 mins
Observation
30 mins – 1 hours
Est. Cost
$400 – $1,800
Department
Ophthalmology
Who Is This For
Is Lacrimal Probing and Intubation Right for You?
Good Candidates
- CNLDO unresponsive to lacrimal sac massage for 3-6 months, in infants aged 6-18 months
- CNLDO with persistent epiphora and discharge beyond 12-18 months of age
- Post-infectious or post-inflammatory lacrimal stenosis after acute dacryocystitis has resolved
- Adults with incomplete canalicular or nasolacrimal duct stenosis from trauma or chronic inflammation
- Partial lacrimal passage obstruction confirmed by lacrimal irrigation, requiring dilation
May Not Be Suitable
- Active acute dacryocystitis with uncontrolled local infection
- Complete fibrotic lacrimal occlusion where a probe cannot be passed (requires DCR)
- Punctal agenesis or congenital canalicular aplasia
- General health precluding anesthesia (pediatric general anesthesia risk must be assessed)
- Nasal cavity mass or severe septal deviation obstructing the nasolacrimal duct outlet
Step-by-Step Process
How Lacrimal Probing and Intubation Works
Anesthesia
Children receive general anesthesia (inhalation induction) to ensure immobility and procedural precision. Cooperative older children and adults may undergo the procedure under topical anesthesia (proparacaine) combined with punctal local infiltration.
Punctal Dilation
The lacrimal punctum is gently dilated with a punctal dilator to allow smooth probe passage without risk of punctal laceration.
Probe Insertion and Duct Opening
An appropriately sized Bowman probe is inserted vertically through the upper or lower punctum for approximately 2 mm, then rotated 90° horizontally and advanced along the canaliculus to the lacrimal sac, then directed inferiorly to perforate the obstructing membrane (typically the membranous lower end of the nasolacrimal duct) into the nasal cavity. A 'give' or 'drop' sensation confirms successful entry.
Irrigation Confirmation
After probe withdrawal, the lacrimal system is irrigated with saline; free flow into the nasal cavity (observed as swallowing in infants or saline emerging from the nares) confirms successful probing.
Silicone Tube Intubation (if indicated)
If the obstruction is severe or re-stenosis is anticipated, a silicone intubation tube is threaded through the probe-created pathway, secured with a knot at the medial canthus, and left in place for 3-6 months before elective clinic removal.
Postoperative Care
Antibiotic eye drops are prescribed. Aftercare instructions are provided to the family and a follow-up schedule is arranged.
Most patients achieve resolution with a single probing session; success rates reach 90-95% in appropriately aged infants. A second probing or tube intubation is considered if the first attempt fails. Adults with repeated probing failure should be referred for dacryocystorhinostomy (DCR). Patients with intubation tubes require a return visit for removal at 3-6 months.
Cost Information
Cost Estimate for Lacrimal Probing and Intubation
Estimated Price Range
$400 – $1,800
What's Included
Public tier-3A International Medical Department: approximately ¥3,000-6,000 (children with light sedation), with silicone tube intubation approximately ¥5,000-9,000; premium private eye centers: approximately ¥6,000-12,000 (including comprehensive dacryocystography assessment).
Before Your Visit
What to Prepare
Required Tests & Examinations
If you already have recent valid test results, bring the reports. If not, these assessments can usually be completed in China before the procedure.
Lacrimal irrigation (confirm site and degree of obstruction; assess punctal and canalicular patency)
Slit-lamp examination (assess punctal morphology, conjunctiva, and cornea)
Nasal endoscopy or nasal inspection (exclude nasal mass; assess inferior meatus anatomy)
Lacrimal sac ultrasound or CT dacryocystography (complex cases or re-probing after prior failure)
Pediatric pre-anesthesia workup (blood count, ECG, anesthesia consultation)
Documents & Materials to Bring
Required to Bring
Prior lacrimal irrigation records and investigation reports
Child's recent physical examination and vaccination records (required for general anesthesia)
Allergy and medication history (especially anticoagulants)
Passport and valid visa
Companion & Support
A parent or guardian must accompany all pediatric patients undergoing general anesthesia. The child must be observed for at least 30-60 minutes post-anesthesia until fully alert with stable vital signs before discharge. Adult patients under local anesthesia benefit from a companion for transportation.
After Treatment
Recovery & Follow-Up
Apply prescribed antibiotic eye drops for 1-2 weeks post-procedure to prevent infection
Children should be discouraged from rubbing their eyes; parents may need to use elbow restraints temporarily to prevent accidental tube dislodgement
If the silicone tube migrates out of the eye, seek prompt medical attention — do not attempt self-adjustment
Significant reduction in tearing and discharge indicates a successful result; persistent symptoms warrant early review
Avoid vigorous eye rubbing and contact sports during the tube-indwelling period to minimize accidental displacement
Continue follow-up for 1-3 months after tube removal to confirm sustained patency
Follow-Up Schedule
Review at 1 week post-procedure to assess lacrimal patency and wound healing. Intubated patients require monthly follow-up; a final review 1-3 months after tube removal confirms sustained patency.
Related Conditions
Conditions This Procedure Treats
Ready to Plan Lacrimal Probing and Intubation in China?
Let Carevia help you find the right hospital, coordinate your treatment, and arrange every detail of your medical trip.
Frequently Asked Questions
Need personalized guidance?
Our care coordinators can help you assess whether this procedure fits your situation.
Contact Us