Corneal Cross-Linking (CXL)
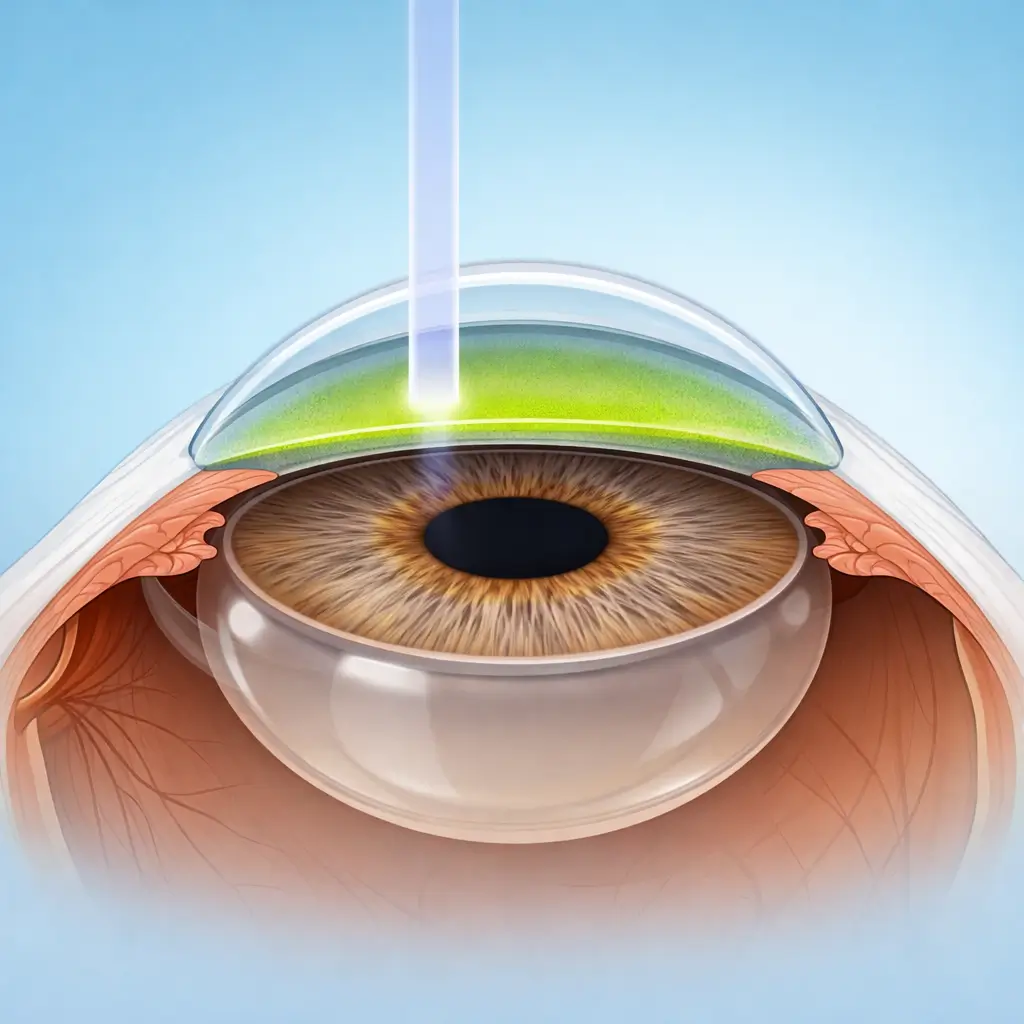
Riboflavin (vitamin B2) photosensitizer combined with UVA irradiation generates reactive oxygen species that form new covalent cross-links between corneal collagen fibers, increasing biomechanical strength and halting the progression of keratoconus.
Corneal Collagen Cross-Linking (CXL) is the only treatment with robust clinical evidence for halting keratoconus progression. Keratoconus is a degenerative corneal ectasia in which loss of covalent bonds between collagen fibrils progressively weakens the cornea, causing it to thin and adopt an asymmetric conical shape that can progress to requiring corneal transplantation if left untreated. In CXL, riboflavin solution is applied to the de-epithelialized stromal surface (standard epithelium-off CXL) or penetrates through intact epithelium (transepithelial/epithelium-on CXL). UVA irradiation at 365-370 nm then activates riboflavin to generate reactive oxygen species (ROS) that catalyze the formation of new covalent cross-links between collagen fibrils, increasing corneal stiffness by approximately 300% and arresting or substantially slowing ectatic progression. The evidence-based standard Dresden protocol (epithelium-off) involves 30 minutes of 0.1% riboflavin soaking followed by 3 mW/cm² UVA irradiation for 30 minutes (total dose 5.4 J/cm²). Accelerated CXL (e.g., 9 mW/cm² for 10 minutes; same total dose) shortens procedural time with comparable long-term outcomes. Transepithelial CXL preserves the epithelium for a more comfortable recovery but has lower riboflavin stromal penetration efficiency; some studies suggest marginally lower stabilization efficacy. The primary goal is stabilization, not reversal — though many patients experience modest improvement in corneal curvature (mean reduction ~1-2 D) and some visual improvement. Patients with residual refractive error after confirmed stabilization may proceed to ICL implantation or specialty contact lens fitting.
Quick Reference
Treatment
1 hours – 1.5 hours
Observation
1 hours – 2 hours
Est. Cost
$1,000 – $3,700
Department
Ophthalmology
Who Is This For
Is Corneal Cross-Linking (CXL) Right for You?
Good Candidates
- Progressive keratoconus confirmed by serial imaging (≥1 D increase in max K or ≥2% decrease in thinnest-point pachymetry over 12-24 months)
- Young patients (<30 years) with keratoconus at high risk of rapid progression
- Thinnest corneal point ≥400 μm (safety threshold for epithelium-off CXL to protect endothelium)
- Early-to-moderate keratoconus with correctable vision
- Iatrogenic corneal ectasia after LASIK or other refractive procedures
May Not Be Suitable
- Thinnest corneal point <400 μm (post-de-epithelialization residual stroma too thin; endothelial damage risk)
- Active corneal infection, significant corneal scarring, or corneal neovascularization
- Advanced keratoconus (Kmax >58 D or uncorrectable vision) — corneal transplantation is more appropriate
- Pregnancy or breastfeeding (limited riboflavin safety data)
- Severe dry eye or ocular surface disease that impairs epithelial healing
Step-by-Step Process
How Corneal Cross-Linking (CXL) Works
Preparation and Topical Anesthesia
Topical anesthetic drops (proparacaine) are instilled. A lid speculum is placed. The central 8 mm treatment zone is marked.
Epithelial Debridement (standard epithelium-off CXL)
The central 8 mm of corneal epithelium is removed mechanically (blunt spatula) or with 20% ethanol (20-second exposure, then BSS rinse), exposing the anterior stroma. Peripheral epithelium is preserved to support healing.
Riboflavin Saturation
0.1% riboflavin solution (in dextran) is applied topically every 2-5 minutes for 30 minutes until the stroma is fully saturated. Visualization of a yellow-green fluorescent signal in the anterior chamber under slit-lamp UV confirms adequate stromal penetration (~200-250 μm depth).
UVA Irradiation
A calibrated UVA source (365-370 nm; 3 mW/cm² for standard protocol or 9 mW/cm² for accelerated protocol) is positioned over the central 8 mm treatment zone. Riboflavin drops are supplemented every 2 minutes to maintain stromal hydration throughout irradiation. Standard protocol: 30 minutes (total dose 5.4 J/cm²). Accelerated protocol: 10 minutes (same total dose).
Completion and Wound Care
The ocular surface is copiously irrigated with BSS. A large-diameter bandage contact lens is placed (to promote epithelial healing and reduce pain). Antibiotic drops are instilled and oral analgesics are prescribed (pain can be significant for 1-3 days post-de-epithelialization). The patient returns in 3-5 days for epithelial healing assessment and contact lens removal.
CXL is a single treatment per eye. Bilateral keratoconus is treated in staged sessions 1-3 months apart. Biomechanical stabilization is complete at 3-6 months; final topographic changes manifest over 12-18 months.
Cost Information
Cost Estimate for Corneal Cross-Linking (CXL)
Estimated Price Range
$1,000 – $3,700
What's Included
Public tier-3A International Medical Department: standard epi-off CXL approximately ¥7,000-12,000 per eye, ¥12,000-18,000 both eyes. Premium private eye centers: standard or accelerated CXL approximately ¥12,000-18,000 per eye, ¥18,000-25,000 both eyes, including comprehensive Pentacam corneal tomography, systematic follow-up planning, and more comfortable environment. Some facilities offer CXL+ICL combined packages.
Before Your Visit
What to Prepare
Required Tests & Examinations
If you already have recent valid test results, bring the reports. If not, these assessments can usually be completed in China before the procedure.
Corneal tomography (Pentacam/Orbscan — curvature maps, pachymetry, anterior and posterior surface morphology; the cornerstone of keratoconus diagnosis and progression monitoring)
Thinnest-point pachymetry (confirm ≥400 μm for CXL safety)
Best spectacle-corrected visual acuity (BSCVA — functional baseline)
Slit-lamp examination (Vogt's striae, Fleischer ring, corneal scarring)
Intraocular pressure (rule out elevated IOP)
Corneal endothelial cell count (assess endothelial safety for CXL)
Documents & Materials to Bring
Required to Bring
Serial corneal tomography reports (Pentacam/Orbscan — ideally ≥2 longitudinal scans demonstrating progression)
Corneal topography comparison series from the past 1-2 years (document progression)
Best corrected visual acuity records
Passport and valid visa
Post-contact-lens-free period examination data (RGP/orthokeratology lens discontinuation ≥1 month)
After Treatment
Recovery & Follow-Up
Days 1-3 after epithelium-off CXL are the most uncomfortable: significant eye pain, photophobia, and tearing — rest, keep eyes closed, and take oral analgesics regularly
Do not remove the bandage contact lens yourself — return for the scheduled visit (day 3-5) for clinician removal
After epithelial healing (~1 week) symptoms improve substantially, but vision may fluctuate for 3-6 months during corneal remodeling
Apply prescribed antibiotic drops (~1-2 weeks) and preservative-free artificial tears (several months) as directed
A transient increase in corneal curvature in the first few months ('early CXL response') is normal before stabilization occurs
Once stabilized, residual refractive error can be addressed with RGP lenses, scleral lenses, or ICL implantation
Follow-Up Schedule
Day 3-5 (epithelial healing check, bandage lens removal), then month 1, month 3, month 6, and year 1 — with serial corneal tomography to monitor curvature and thickness. Annual follow-up thereafter to confirm ongoing stability.
Related Conditions
Conditions This Procedure Treats
Ready to Plan Corneal Cross-Linking (CXL) in China?
Let Carevia help you find the right hospital, coordinate your treatment, and arrange every detail of your medical trip.
Frequently Asked Questions
Need personalized guidance?
Our care coordinators can help you assess whether this procedure fits your situation.
Contact Us